HISTORY:
A 20+ year old male presents with an increasing number of papules and nodules on the ears and upper limbs in the last 3 months. Associated symptoms include erythema and pruritus, not relieved by oral steroids. Pertinent negatives include fever, fatigue, myalgia, lymphadenopathy, and changes in sensation. The patient moved from Micronesia to the United States 1.5 years ago.
What is the most likely diagnosis?



DIAGNOSIS & CASE SUMMARY:
Leprosy (lepromatous leprosy)
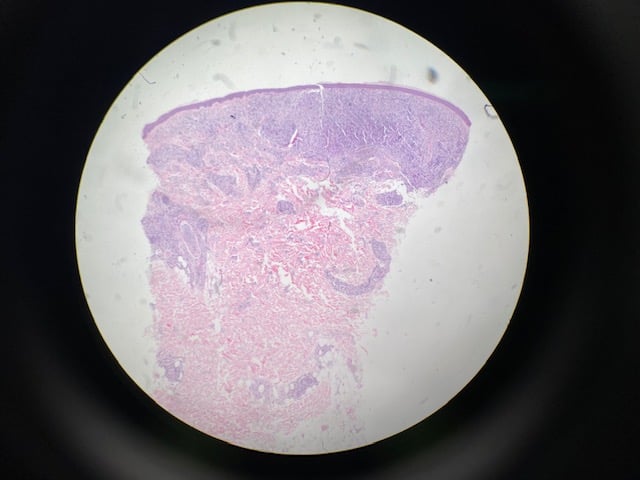
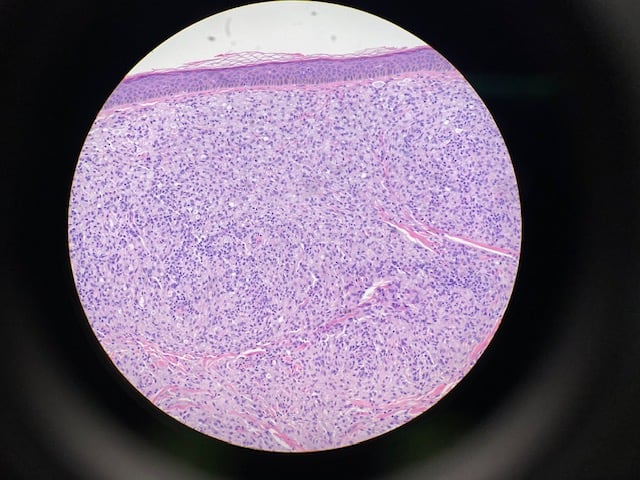
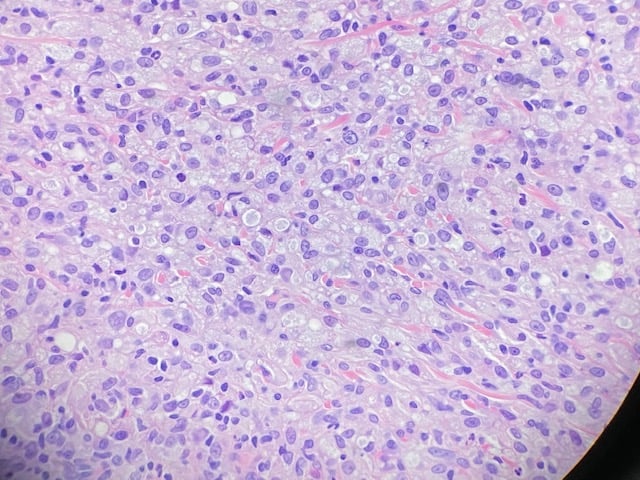
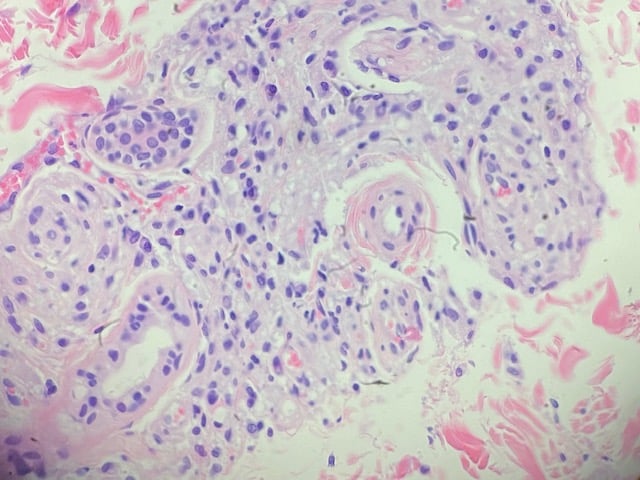
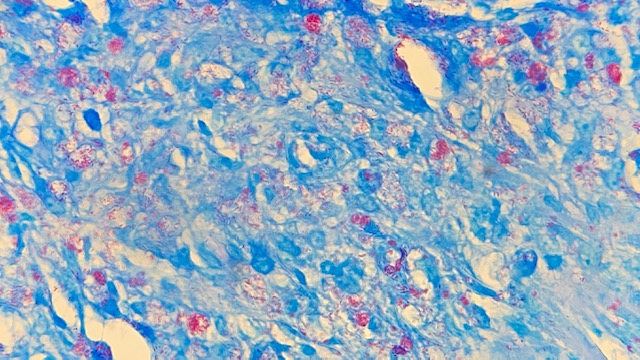
Two biopsies from the right and left upper arms show granulomatous dermatitis with numerous bacilli on AFB stain. The histopathologic differential diagnosis includes lepromatous leprosy and mycobacteria infection. Given the granulomas with foamy histiocytes and infiltrate along nerves and adnexal structures, lepromatous leprosy was favored. The PAS, GMS, and mucicarmine stain fail to show Cryptococci in the granulomas. Paraffin embedded tissue block was sent to National Hansen’s Disease (Leprosy) Program for Mycobacterium leprae PCR which was positive.
Leprosy is an infectious disease caused by the acid-fast bacillus Mycobacetrium leprae, an intracytoplasmic parasite of macrophages and Schawnn cells. The average incubation period is 4-10 years. It is slowly progressive and characterized by granulomas in the skin and peripheral nerves. The majority of people exposed do not develop disease due to genetic (HLA type) and environmental factors.
Leprosy is divided into two major forms- lepromatous leprosy (Th2 mediated), which usually has numerous, symmetrically distributed, macules, papules, and nodules with diffuse infiltration and numerous acid-fast bacilli found in lesions and tuberculoid leprosy (Th1 mediated), which usually has one to a few anesthetic, infiltrated plaques with raised borders and central hypopigmentation and few to no acid-fast bacilli found in lesions. Treatment requires a multidrug regimen for 1-2 years.
FOLLOW-UP:
Treatment plan discussed with National Hansen’s Disease (Leprosy) Program as follows: rifampin 600 mg monthly, moxifloxacin 400 mg monthly, minocycline 100 mg monthly, and vitamin D 50,000 units monthly x24 months with directly observed therapy in office. The patient is currently undergoing care at Forefront Dermatology.
Reference: Ramos-e-Silva, Marcia, and Maria Cristina Ribeiro de Castro. “Mycobacterial Infections.” Dermatology, Third ed., vol. 2, Elsevier Limited, 2012, pp. 1221–1242.