HISTORY:
This 50+ year-old gentleman presented with a papule on the left forehead. He has a previous history of cutaneous squamous cell carcinoma and basal cell carcinoma. There was no significant medical history and the surgical history is bowel resection for malignancy. A shave biopsy was performed.
QUESTION:
What syndrome should be considered?


Chrimogranin
Synaptophysin
Cytokeratin
TTF1
CDX2
ANSWER
Carcinoid syndrome
PATHOLOGY
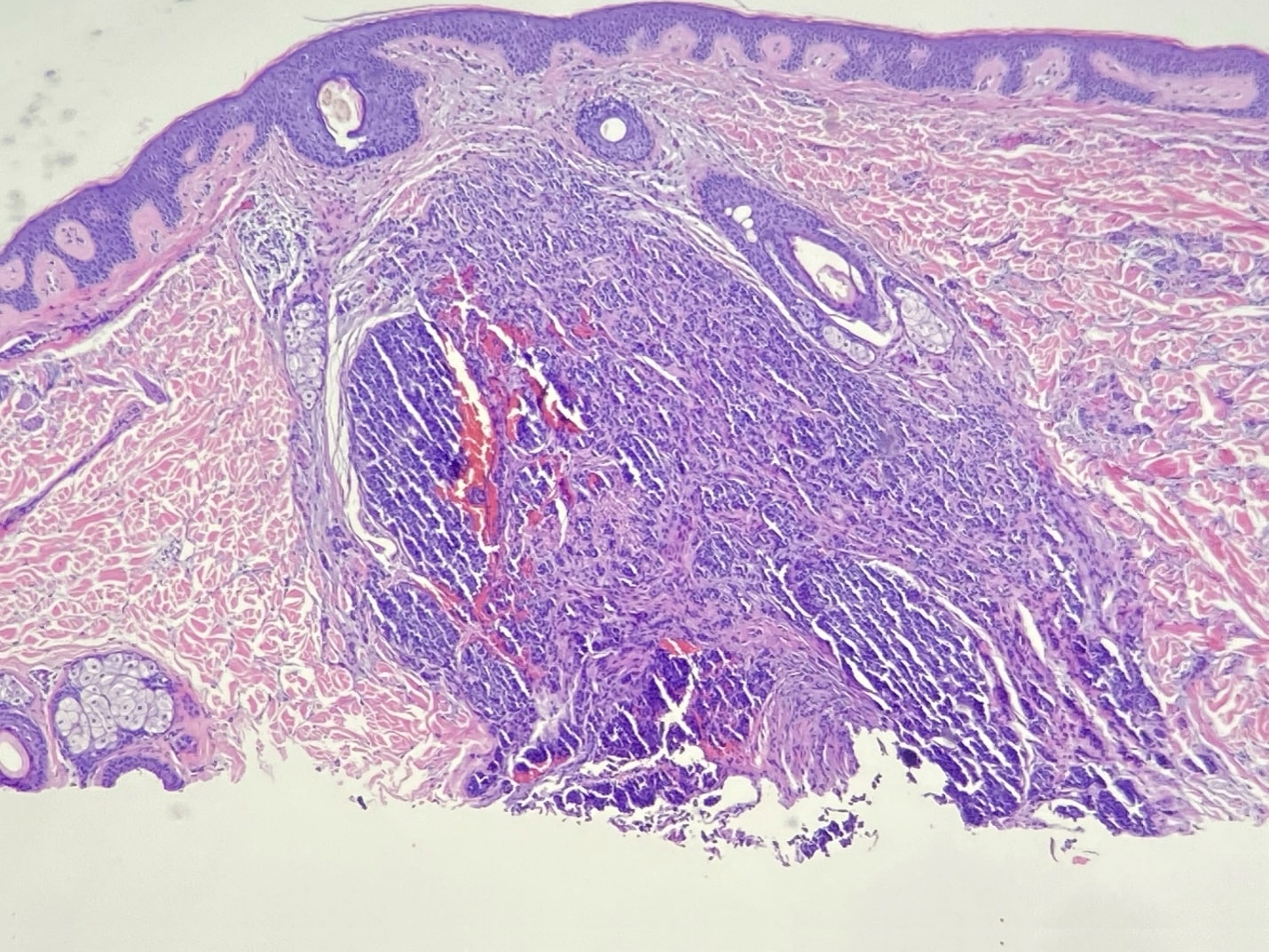
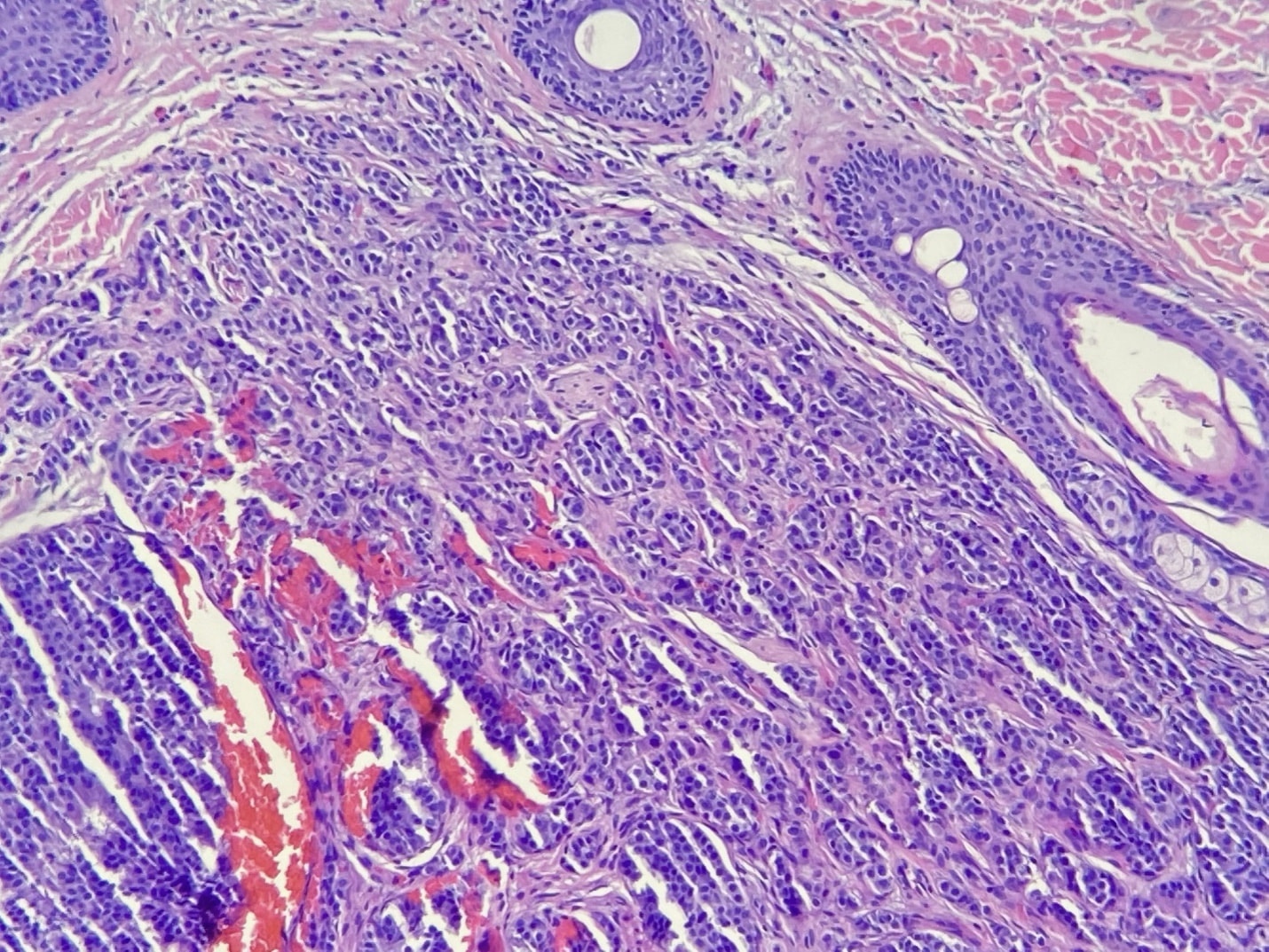
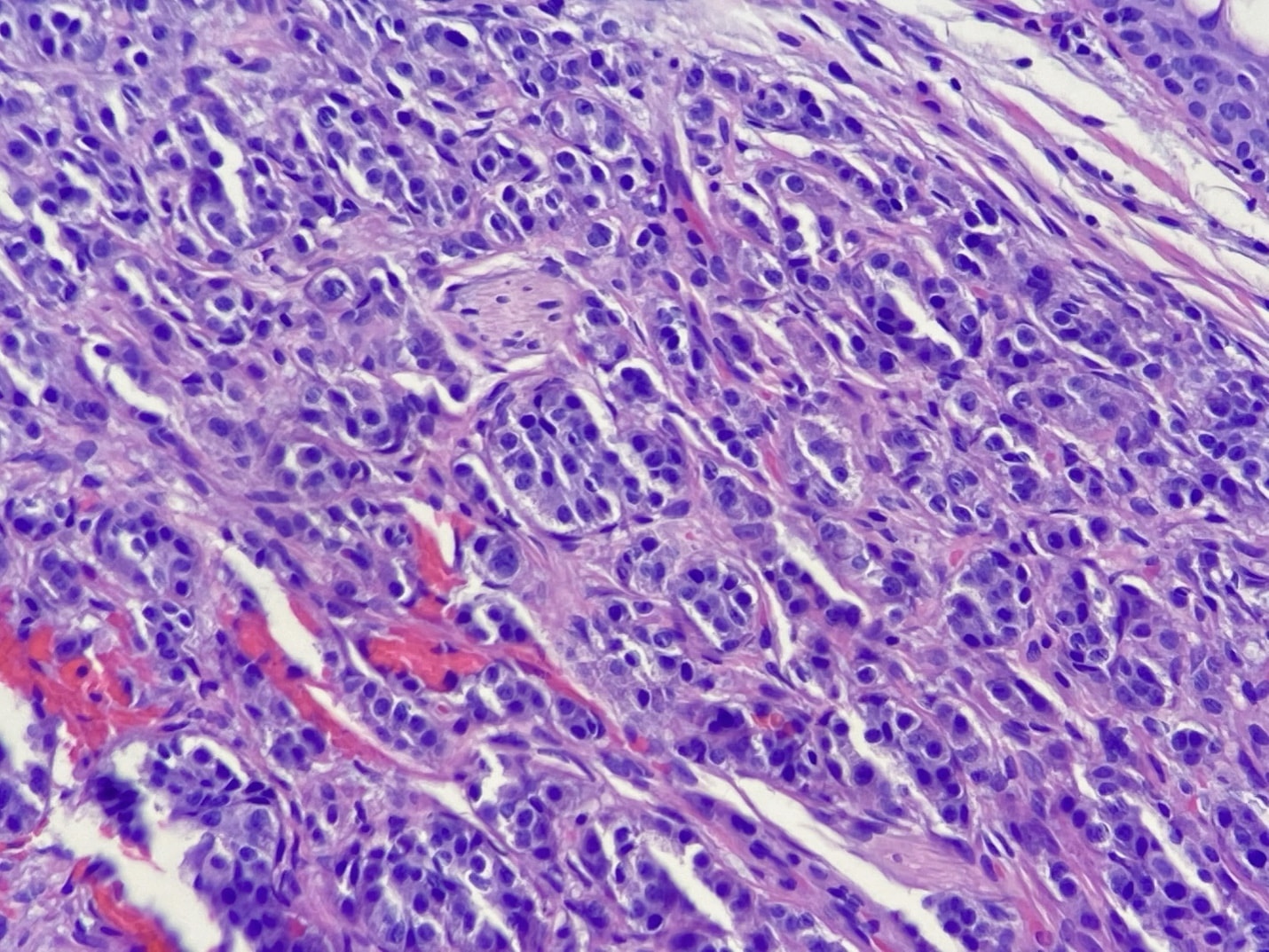
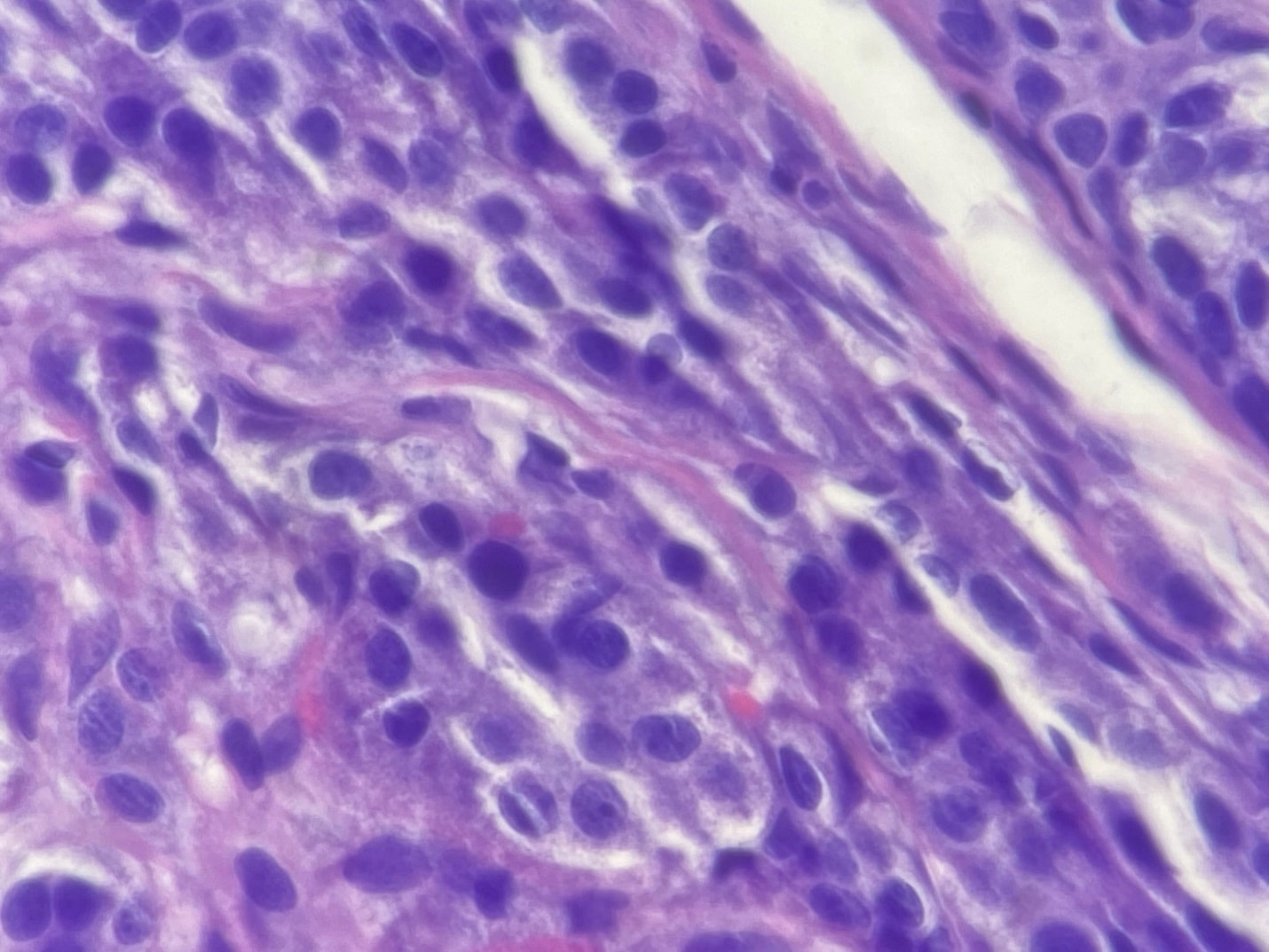
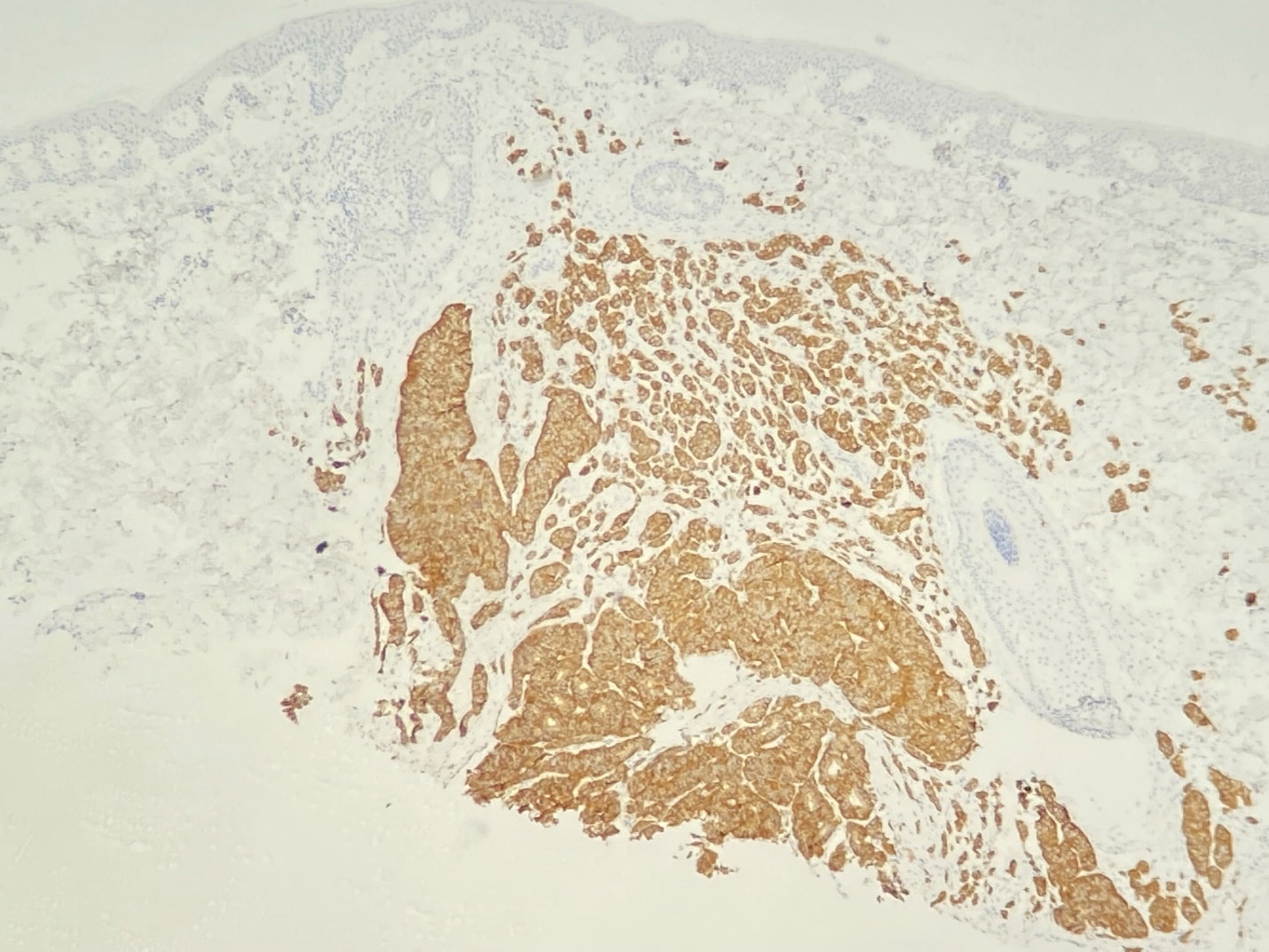
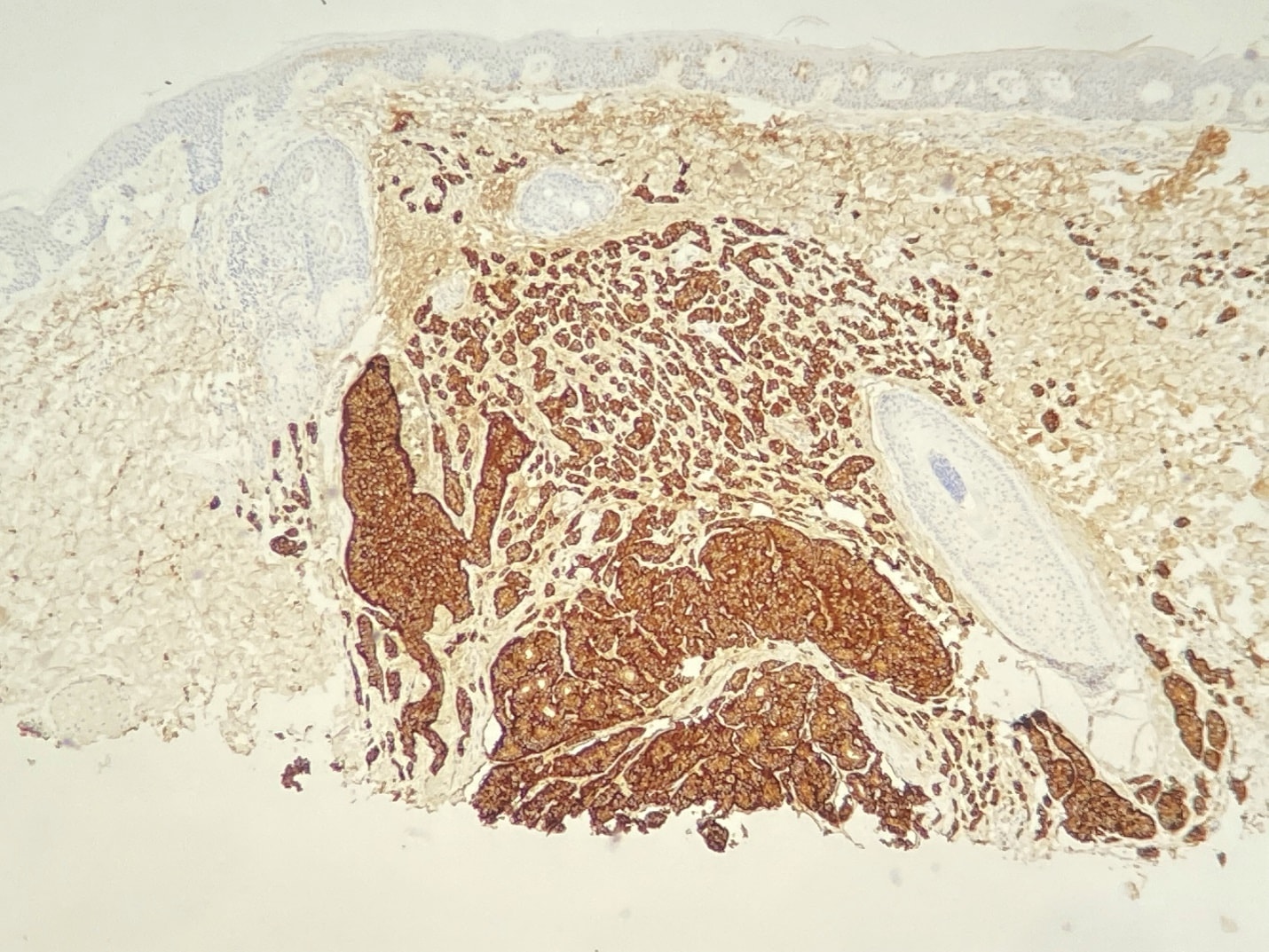
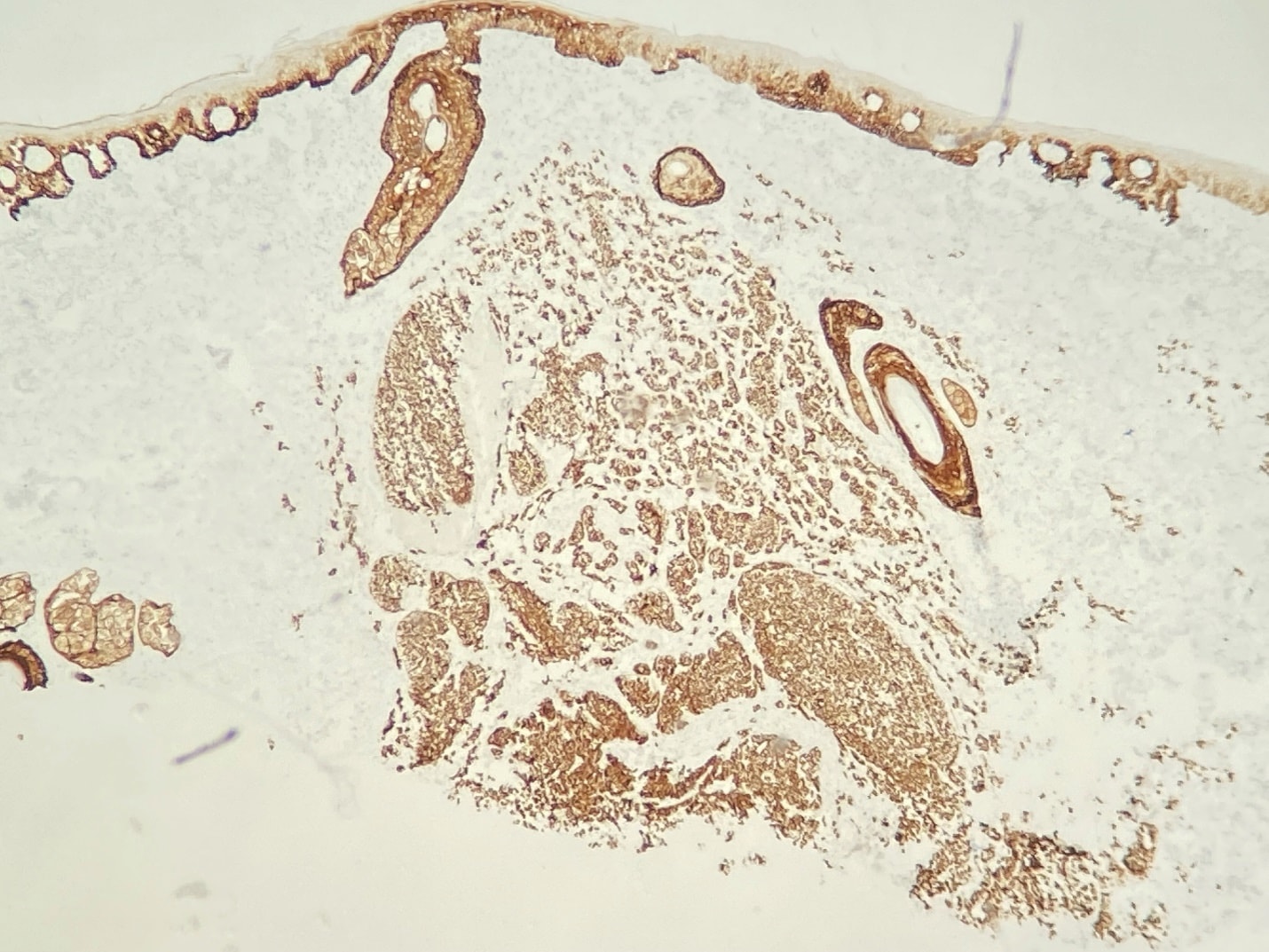
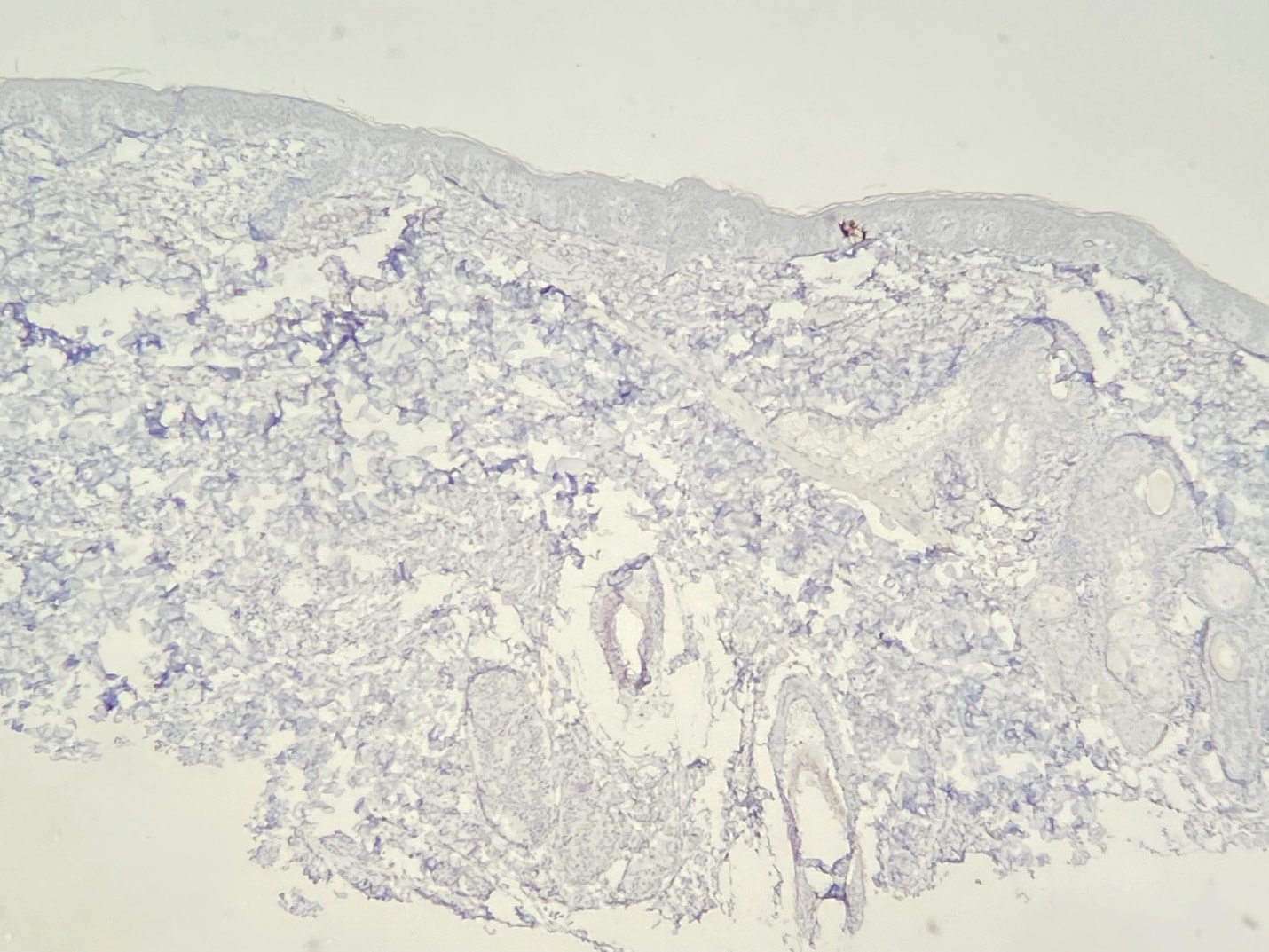
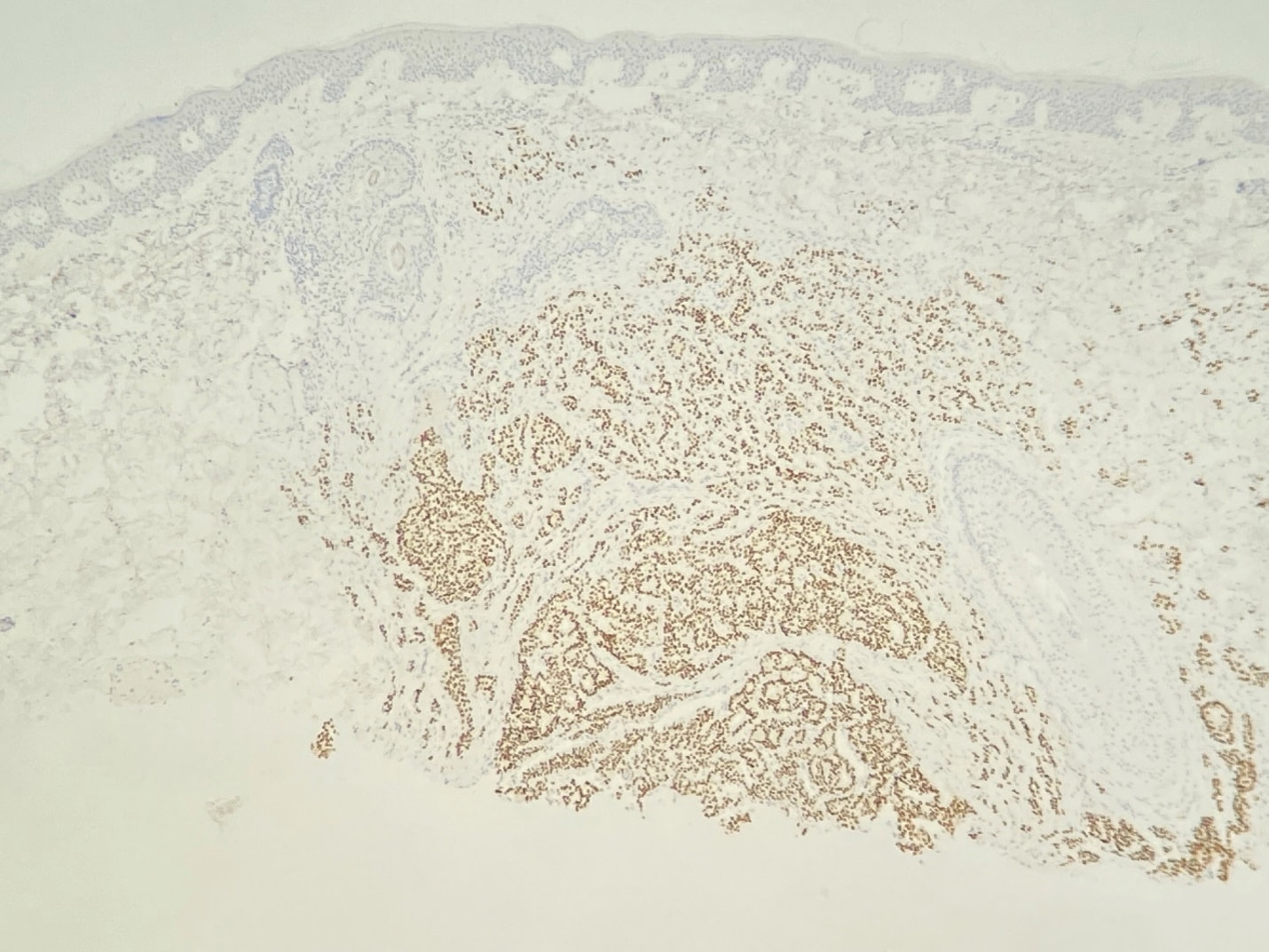
The shave biopsy of the forehead papule revealing a monotonous proliferation of epithelioid cells with an organoid growth pattern. There is no necrosis, and mitotic figures are not evident. The nuclei are round, with “salt and pepper” chromatin, giving the impression of carcinoid tumor. The neoplasm was diffusely and uniformly positive for cytokeratin cocktail (AE1/AE3), as well as chromogranin and synaptophysin. The combination of morphology and immunophenotype is diagnostic of carcinoid tumor. TTF-1 was negative and CDX2 was uniformly positive. The large majority of carcinoid tumors in the skin are metastatic, with only a handful of possible primary cutaneous carcinoids reported in the literature. Most carcinoids arise from pulmonary or gut primary sites. TTF-1 has good sensitivity and excellent specificity for pulmonary carcinoids, and CDX2 has good sensitivity and excellent specificity for gastrointestinal carcinoids. The expression of CDX2 in this case is consistent with metastatic gastrointestinal carcinoid tumor.
CASE SUMMARY
The patient did not provide the pertinent history at the initial visit because he did not think that carcinoid tumors could involve the skin. Subsequent questioning revealed that he was first diagnosed in 2009 (with an extensive workup at the local university), and endoscopy revealed numerous tumors that required intestinal resection. Everything went smoothly until 2015 when he began having symptoms of “carcinoid syndrome”: flushing, sweating, GI symptoms, etc. The tumor(s) had metastasized to the liver. He was treated with radiation and octreotide injections, and his condition stabilized, but he was still experiencing symptoms. He had a PET scan, which at the time of this write up has yet to be interpreted. As you can see from the clinical photographs, his face is quite flushed.
Carcinoid syndrome is the result of serotonin, which is produced by carcinoid tumors. Symptoms include flushing, diarrhea, abdominal pain, bronchoconstriction, and carcinoid heart disease (valvular fibrosis). Most patients with carcinoid tumors never develop carcinoid syndrome. The liver is remarkably effective at metabolizing serotonin. When the metastatic tumor burden becomes large enough, it overwhelms the liver’s ability to deal with the excess serotonin, and “carcinoid syndrome” develops. This is uncommon, and only affecting about 1000 patients in the US annually.
There have been cases where the lesions have been misdiagnosed, as adnexal poroid neoplasms and other cutaneous neoplasms, so a high degree of suspicion and application of pertinent immunohistochemistry tests will often lead to the correct diagnosis. We found this case to be highly interesting because, although our dermatopathologist has seen many cases of visceral carcinoid, this cutaneous metastasis is a first.
FOLLOW-UP
The patient has been seen again for follow up and unfortunately his PET scan revealed “widespread disease,” according to the patient. He is to be evaluated for further treatment at the university health system in the near future.
By: Dr. Joseph Hanson, MD; Dr. Doug Hansen, MD